A
Figure 2.
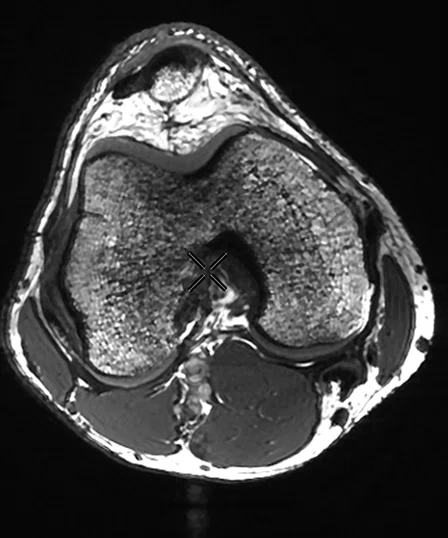
3D Fiesta-C images of the knee, (A) Axial and (B) sagittal acquired on the SIGNA 7.0T at the University of Iowa MRRF.
B
Figure 2.
3D Fiesta-C images of the knee, (A) Axial and (B) sagittal acquired on the SIGNA 7.0T at the University of Iowa MRRF.
A
Figure 3.
(A) MP-RAGE with a 0.5 mm isotropic acquisition and (B) T2 FSE with high acoustic noise reduction.
B
Figure 3.
(A) MP-RAGE with a 0.5 mm isotropic acquisition and (B) T2 FSE with high acoustic noise reduction.
‡ For research use only. Not cleared for clinical use in the US or any other country.
‡‡ Not yet CE marked. Not available for sale in all regions.
‡‡‡ Technology in development that represents ongoing research and development efforts. These technologies are not products and may never become products. Not for sale. Not cleared or approved by the US FDA or any other global regulator for commercial availability.
‡‡‡‡ Technology in development and not cleared for clinical use on SIGNA™ 7.0T in the US or any other country.
A
Figure 1.
The team at MRRF celebrates the grand reopening following the upgrade to SIGNA™ 7.0T. Note the system as pictured has the previous Discovery MR950 covers.




result
PREVIOUS
${prev-page}
NEXT
${next-page}
Subscribe Now
Manage Subscription
FOLLOW US
Contact Us • Cookie Preferences • Privacy Policy • California Privacy PolicyDo Not Sell or Share My Personal Information • Terms & Conditions • Security
© 2024 GE HealthCare. GE is a trademark of General Electric Company. Used under trademark license.

SPOTLIGHT
An ultra-high-field upgrade advancing the understanding of disease
An ultra-high-field upgrade advancing the understanding of disease
Located in America’s heartland, the University of Iowa MR Research Facility (MRRF) is at the forefront of high-field, neuroscience-focused research. The center’s Discovery™ MR950‡, a research-based 7.0T MR system, was recently upgraded to the SIGNA™ 7.0T‡‡, GE Healthcare’s powerful new platform for advancing neurological research and clinical translation.
Located in America’s heartland, the University of Iowa MR Research Facility (MRRF) is at the forefront of high-field, neuroscience-focused research. The center’s Discovery™ MR950‡, a research-based 7.0T MR system, was recently upgraded to the SIGNA™ 7.0T‡‡, GE Healthcare’s powerful new platform for advancing neurological research and clinical translation.
The MRRF also has a SIGNA™ Premier 3.0T and GE MR901 7.0T scanner (preclinical). In early 2023, the center will install GE’s investigational high-performance Microstructure Anatomy Gradient for Neuroimaging with Ultrafast Scanning (MAGNUS)‡‡‡, a gradient platform for the SIGNA™ Premier 3.0T system.

A
Figure 1.
The team at MRRF celebrates the grand reopening following the upgrade to SIGNA™ 7.0T. Note the system as pictured has the previous Discovery MR950 covers.
The addition of 7.0T MR at the MRRF has not just opened up new capabilities in research, but has helped attract some of the brightest scientists, physicists and clinicians to the University of Iowa. The MRRF is served by six faculty members with expertise in MR physics and reconstruction. They have six NIH-funded R01 grants and one S10 grant. There are three scientific staff members within the facility, four MR technologists and one support engineer. The MRRF has seven students and two post-doctoral fellows working with the faculty members. On an annual basis, the MRRF operates to serve approximately 30 NIH-funded grants and an additional 15 other projects.
With the Discovery™ MR950, MRRF has studied vessel wall characterization and enhancement to potentially identify people susceptible to aneurysms, phosphorous spectroscopy to examine adenosine triphosphate as well as pH in bipolar disorder, and evaluate terazosin as a potential treatment for Parkinson’s disease.
Also in Parkinson’s disease, the center is aiming to identify the volume of substantia nigra and integrate this information with diffusion imaging. In breast cancer patients, another study is examining the impact of chemotherapy on the brain with quantitative susceptibility mapping (QSM)‡‡‡‡-based measures and MR spectroscopy. In pediatrics, studies include task-based and resting-state fMRI in attention deficit/hyperactivity disorder and autistic subjects. In these fMRI studies, Vincent Magnotta, PhD, Director of the MRRF and Professor of Radiology-Division of Neuroradiology at the University of Iowa, will attain 1.5 mm isotropic functional imaging data with the SIGNA™ 7.0T.
The key reason for upgrading to SIGNA™ 7.0T was the advancement in the system’s hardware and software, explains Dr. Magnotta. Among other improvements, the SIGNA™ 7.0T brings new state-of-the-art features, such as AIR™ Recon DL, and a level of application commonality with the SIGNA™ Premier 3.0T system.
“The gradient performance of SIGNA™ 7.0T is top of the line,” he says. “We have improved RF capabilities and many new software features will provide us a common advanced scanning platform across systems. Overall, the workflow is substantially improved and that will facilitate scanning at 7.0T.”
In addition to neuro-based applications, Dr. Magnotta says the SIGNA™ 7.0T has demonstrated a drastic improvement in MSK imaging, particularly in the knee, which he attributes to coil and software advancements.
“It was amazing how much the knee imaging improved,” Dr. Magnotta says. “We are definitely much further ahead than I would have expected with a new system install. I was anticipating more work to get it up and running.”
A

B
Figure 2.
3D Fiesta-C images of the knee, (A) Axial and (B) sagittal acquired on the SIGNA 7.0T at the University of Iowa MRRF.
In just the first week after the installation, the team at MRRF has acquired 0.5 mm isotropic MP-RAGE brain images and is currently testing how far they can push AIR™ Recon DL, particularly to reduce noise in white-matter-nulled acquisitions to identify deep subnuclei in the thalamus. This latter technique could be an alternative to FLAIR imaging, he adds.
“With 7.0T, we can enhance spatial resolution in gray/white matter differentiation, whether that is with IR prep or Cube-based variable flip angle sequences, to provide additional anatomic information that we can’t get at 3.0T,” Dr. Magnotta adds.

A

B
Figure 3.
(A) MP-RAGE with a 0.5 mm isotropic acquisition and (B) T2 FSE with high acoustic noise reduction.
He is also excited to explore the different imaging capabilities of 7.0T and compare it to the MAGNUS 3.0T platform once it is installed at MRRF.
“There will be some things we can do on MAGNUS that are more challenging at 7.0T due to gradient performance, as well as some physical properties, such as faster T2 decay at 7.0T compared to 3.0T,” Dr. Magnotta explains. “There are some really exciting opportunities with MAGNUS in diffusion imaging and white matter assessment, coupled with high-resolution imaging, that may provide an extraordinary understanding of what is happening in the brain across different clinical indications or diseases.
“There are some studies that are just ripe for 7.0T,” Dr. Magnotta adds. “We have new data from SIGNA™ 7.0T that also suggests we may be able to distinguish the head of the hippocampus from the amygdala, which has traditionally not been possible. This has implications for studies of Alzheimer’s disease and also may inform when to start treatment. There is so much room for growth and advancement with 7.0T.”
