A-1
Figure 2.
A 38-week pregnant woman was diagnosed with fetal bowel dilatation from the fetal colon to the rectum on ultrasound and was referred to MR. AIR™ Recon DL was utilized for the examination. (A) T2 SSFSE and (B) FIESTA were both acquired with a slice thickness of 5.0 mm.
B-1
Figure 2.
A 38-week pregnant woman was diagnosed with fetal bowel dilatation from the fetal colon to the rectum on ultrasound and was referred to MR. AIR™ Recon DL was utilized for the examination. (A) T2 SSFSE and (B) FIESTA were both acquired with a slice thickness of 5.0 mm.
A-2
Figure 2.
A 38-week pregnant woman was diagnosed with fetal bowel dilatation from the fetal colon to the rectum on ultrasound and was referred to MR. AIR™ Recon DL was utilized for the examination. (A) T2 SSFSE and (B) FIESTA were both acquired with a slice thickness of 5.0 mm.
B-2
Figure 2.
A 38-week pregnant woman was diagnosed with fetal bowel dilatation from the fetal colon to the rectum on ultrasound and was referred to MR. AIR™ Recon DL was utilized for the examination. (A) T2 SSFSE and (B) FIESTA were both acquired with a slice thickness of 5.0 mm.
A
Figure 3.
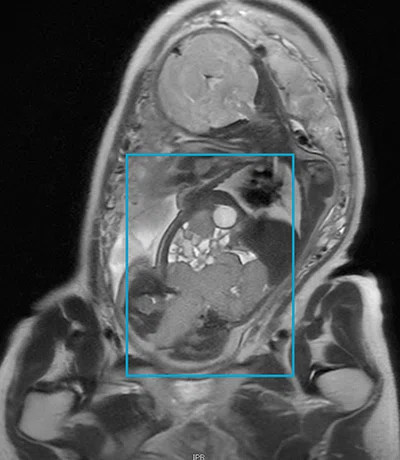
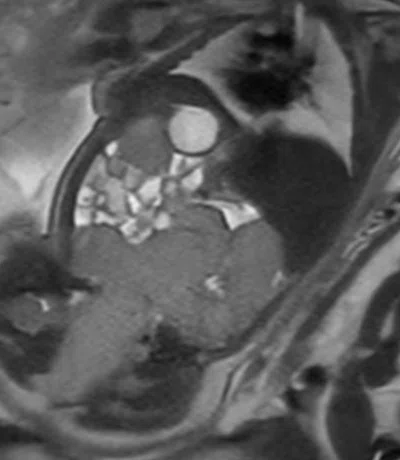
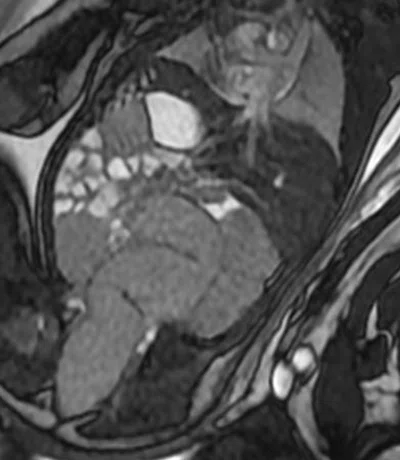
With thinner slice thickness, structures within the placenta and abnormal blood vessels (blue arrow) between the placenta and the muscle layer can be evaluated in more detail. (A) Slice thickness 5.0 mm without AIR™ Recon DL; (B) slice thickness 5.0 mm with AIR™ Recon DL; (C) slice thickness 3.0 mm without AIR™ Recon DL; and (D) slice thickness 3.0 mm with AIR™ Recon DL.
B
Figure 3.
With thinner slice thickness, structures within the placenta and abnormal blood vessels (blue arrow) between the placenta and the muscle layer can be evaluated in more detail. (A) Slice thickness 5.0 mm without AIR™ Recon DL; (B) slice thickness 5.0 mm with AIR™ Recon DL; (C) slice thickness 3.0 mm without AIR™ Recon DL; and (D) slice thickness 3.0 mm with AIR™ Recon DL.
C
Figure 3.
With thinner slice thickness, structures within the placenta and abnormal blood vessels (blue arrow) between the placenta and the muscle layer can be evaluated in more detail. (A) Slice thickness 5.0 mm without AIR™ Recon DL; (B) slice thickness 5.0 mm with AIR™ Recon DL; (C) slice thickness 3.0 mm without AIR™ Recon DL; and (D) slice thickness 3.0 mm with AIR™ Recon DL.
D
Figure 3.
With thinner slice thickness, structures within the placenta and abnormal blood vessels (blue arrow) between the placenta and the muscle layer can be evaluated in more detail. (A) Slice thickness 5.0 mm without AIR™ Recon DL; (B) slice thickness 5.0 mm with AIR™ Recon DL; (C) slice thickness 3.0 mm without AIR™ Recon DL; and (D) slice thickness 3.0 mm with AIR™ Recon DL.
A-1
Figure 4.
(A) In the supine position, the inferior vena cava is compressed (blue arrow), however, (B) in the left lateral decubitus position, the inferior vena cava is not compressed, which can prevent inferior vena cava syndrome. (C) The use of the AIR™ AA Coil allows for positioning in the left lateral decubitus position, providing a more comfortable exam for the patient.
B-1
Figure 4.
(A) In the supine position, the inferior vena cava is compressed (blue arrow), however, (B) in the left lateral decubitus position, the inferior vena cava is not compressed, which can prevent inferior vena cava syndrome. (C) The use of the AIR™ AA Coil allows for positioning in the left lateral decubitus position, providing a more comfortable exam for the patient.
C
Figure 4.
(A) In the supine position, the inferior vena cava is compressed (blue arrow), however, (B) in the left lateral decubitus position, the inferior vena cava is not compressed, which can prevent inferior vena cava syndrome. (C) The use of the AIR™ AA Coil allows for positioning in the left lateral decubitus position, providing a more comfortable exam for the patient.
A-2
Figure 4.
(A) In the supine position, the inferior vena cava is compressed (blue arrow), however, (B) in the left lateral decubitus position, the inferior vena cava is not compressed, which can prevent inferior vena cava syndrome. (C) The use of the AIR™ AA Coil allows for positioning in the left lateral decubitus position, providing a more comfortable exam for the patient.
B-2
Figure 4.
(A) In the supine position, the inferior vena cava is compressed (blue arrow), however, (B) in the left lateral decubitus position, the inferior vena cava is not compressed, which can prevent inferior vena cava syndrome. (C) The use of the AIR™ AA Coil allows for positioning in the left lateral decubitus position, providing a more comfortable exam for the patient.
A
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
B
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
C
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
D
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
E
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
F
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
G
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
H
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.




result
PREVIOUS
${prev-page}
NEXT
${next-page}
Subscribe Now
Manage Subscription
FOLLOW US
Contact Us • Cookie Preferences • Privacy Policy • California Privacy PolicyDo Not Sell or Share My Personal Information • Terms & Conditions • Security
© 2024 GE HealthCare. GE is a trademark of General Electric Company. Used under trademark license.

Yoshiko Ueno, MD, PhD
Kobe University Graduate School of Medicine
—
Kobe, Japan
Shintarou Horii, RT
Kobe University Hospital
—
Kobe, Japan
In Practice
An upgrade facilitating fast, high SNR fetal imaging with greater patient comfort
An upgrade facilitating fast, high SNR fetal imaging with greater patient comfort
Yoshiko Ueno, MD, PhD
Kobe University Graduate School of Medicine
—
Kobe, Japan
Shintarou Horii, RT
Kobe University Hospital
—
Kobe, Japan
Although ultrasound remains the preferred diagnostic imaging study during pregnancy, MR imaging is often ordered after an ultrasound to obtain additional information or detect perinatal development disorders. MR studies offer high spatial resolution to evaluate the volume of amniotic fluid, the placenta’s position, its size and signal intensity in the uterus, the length and anatomy of the umbilical cord, and more.
Kobe University Hospital is the affiliated hospital of Kobe University School of Medicine in Kobe, Japan, and is one of the leading hospitals in Hyogo Prefecture. The hospital receives referrals from many other clinics and hospitals in the region to provide cutting-edge diagnoses and treatments. The MR suite performs 65 MR studies per day, including several exams per week on pregnant women.
The department recently upgraded its SIGNA™ Voyager 1.5T with MR 30 for SIGNA™, adding AIR™ Recon DL to its imaging capabilities and enabling the use of AIR™ Coils. With these technologies, Kobe University Hospital has been able to improve exam speed and comfort when assessing the placenta and fetus. “All of these exams are performed on the SIGNA™ Voyager 1.5T for the safety of pregnant women,” says Shintarou Horii, RT, Kobe University Hospital.
AIR™ Recon DL speeds fetal imaging
The adoption of ultrafast sequences has improved fetal MR by diminishing artifacts caused by fetal motion. Kobe University Hospital utilizes AIR™ Recon DL differently depending upon the sequence: in DWI, it is used to reduce scan time; in single-shot fast spin echo (SSFSE) and FIESTA sequences, it is used to improve image quality. In Horii’s experience, AIR™ Recon DL works well with these sequences and is commonly used in placental examinations. “We use AIR™ Recon DL on High for SSFSE and DWI sequences, and on Medium for FIESTA sequences due to its high original SNR,” he says.
At Kobe, SSFSE is often combined with AIR™ Recon DL to maximize the receive bandwidth with a time echo (TE) of 90 ms. “At 90 ms, it has the best contrast around the placenta, as a result of acquiring images at four different TEs. Shorter TEs are used so that the longer T2 species (like water) do not shine too brightly and the peri-placental area can be easily observed,” says Horii.
Yoshiko Ueno, MD, PhD, radiologist in the Department of Radiology at Kobe University Graduate School of Medicine, said AIR™ Recon DL enables thinner slices of 3 mm, compared to the 10 mm used at other facilities. “By taking thinner-slice images, structures in the placenta, abnormal blood vessels between the placenta and muscle layer, umbilical cord attachment sites, and fetal structures can be evaluated in more detail,” she says.
Image quality has also improved, while acquisition time has been shortened. Now they can capture thin slices without losing SNR. “Before the installation of AIR™ Recon DL, we imaged with thin slices, but the SNR was low due to the thin slices,” adds Dr. Ueno. Now, Dr. Ueno has the best of both – higher SNR in thinner slices.

A

B

C

D

E

F

G

H
Figure 1.
In examinations of the placenta, image quality has improved with AIR™ Recon DL. (A) T2 SSFSE, (B) DWI b1000, (C) T2 SSFSE, and (D) FIESTA, all with 5 mm slice thickness and conventional reconstruction. (E) T2 SSFSE, (F) DWI b1000, (G) T2 SSFSE, and (H) FIESTA, all with 5 mm slice thickness and AIR™ Recon DL.
A-1

B-1
A-2
B-2
Figure 2.
A 38-week pregnant woman was diagnosed with fetal bowel dilatation from the fetal colon to the rectum on ultrasound and was referred to MR. AIR™ Recon DL was utilized for the examination. (A) T2 SSFSE and (B) FIESTA were both acquired with a slice thickness of 5.0 mm.
Flexible comfort for pregnant patients
The MR 30 for SIGNA™ upgrade enabled Kobe University Hospital to implement flexible and lightweight AIR™ Coils. “AIR™ Coils are very well suited for pregnant women’s examinations because they are lightweight and can fit closely to the patient. They are easy to set up, especially since the pregnant woman is placed in the left lateral decubitus position to avoid inferior vena cava syndrome (IVCS),” Horii explains.
Pregnant women in the supine position throughout the MR scan sometimes feel sick due to IVCS and must change positions. “The use of the AIR™ Coils now allows the examination to be performed in the left lateral recumbent position from the beginning, which improves patient comfort,” says Dr. Ueno.
These coils support high image quality, too. “The AIR™ Coils and AIR™ Recon DL have also made it possible to obtain images in the left lateral decubitus position that are comparable in quality to those obtained in the supine position,” adds Dr. Ueno.
Both Dr. Ueno and Horii believe SIGNA™ Voyager 1.5T with MR 30 for SIGNA™ has improved the quality of fetal MR examinations at Kobe University Hospital. “The image quality of the SIGNA™ Voyager 1.5T with the MR 30 for SIGNA™ upgrade is much better, thanks to AIR™ Recon DL,” says Horii.

A

B

C

D
Figure 3.
With thinner slice thickness, structures within the placenta and abnormal blood vessels (blue arrow) between the placenta and the muscle layer can be evaluated in more detail. (A) Slice thickness 5.0 mm without AIR™ Recon DL; (B) slice thickness 5.0 mm with AIR™ Recon DL; (C) slice thickness 3.0 mm without AIR™ Recon DL; and (D) slice thickness 3.0 mm with AIR™ Recon DL.
Figure 4.
(A) In the supine position, the inferior vena cava is compressed (blue arrow), however, (B) in the left lateral decubitus position, the inferior vena cava is not compressed, which can prevent inferior vena cava syndrome. (C) The use of the AIR™ AA Coil allows for positioning in the left lateral decubitus position, providing a more comfortable exam for the patient.
DOWNLOAD ARTICLE HERE
