A
Figure 6.
Claustrophobic patients often cannot breath-hold. Respiratory triggering can be utilized in these patients. (A, B) Images were acquired with Sonic™ DL, 1 R-R, entire HLA stack in 1:20 min.
B
Figure 6.
Claustrophobic patients often cannot breath-hold. Respiratory triggering can be utilized in these patients. (A, B) Images were acquired with Sonic™ DL, 1 R-R, entire HLA stack in 1:20 min.
A
Figure 2.
A 76-year-old male patient with shortness of breath, claustrophobia and arrhythmia with an abnormal echocardiogram. Short axis cine images, (A) FIESTA Cine, (B) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R. In the 3-chamber view images, (D) FIESTA Cine image quality is marred by the severe arrhythmia, which obscures the aortic regurgitant jet. Both the (E) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R, clearly provide better image quality in this patient.
B
Figure 2.
A 76-year-old male patient with shortness of breath, claustrophobia and arrhythmia with an abnormal echocardiogram. Short axis cine images, (A) FIESTA Cine, (B) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R. In the 3-chamber view images, (D) FIESTA Cine image quality is marred by the severe arrhythmia, which obscures the aortic regurgitant jet. Both the (E) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R, clearly provide better image quality in this patient.
C
Figure 2.
A 76-year-old male patient with shortness of breath, claustrophobia and arrhythmia with an abnormal echocardiogram. Short axis cine images, (A) FIESTA Cine, (B) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R. In the 3-chamber view images, (D) FIESTA Cine image quality is marred by the severe arrhythmia, which obscures the aortic regurgitant jet. Both the (E) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R, clearly provide better image quality in this patient.
D
Figure 2.
A 76-year-old male patient with shortness of breath, claustrophobia and arrhythmia with an abnormal echocardiogram. Short axis cine images, (A) FIESTA Cine, (B) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R. In the 3-chamber view images, (D) FIESTA Cine image quality is marred by the severe arrhythmia, which obscures the aortic regurgitant jet. Both the (E) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R, clearly provide better image quality in this patient.
E
Figure 2.
A 76-year-old male patient with shortness of breath, claustrophobia and arrhythmia with an abnormal echocardiogram. Short axis cine images, (A) FIESTA Cine, (B) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R. In the 3-chamber view images, (D) FIESTA Cine image quality is marred by the severe arrhythmia, which obscures the aortic regurgitant jet. Both the (E) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R, clearly provide better image quality in this patient.
A
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.
B
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.
C
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.
D
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.
E
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.
F
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.
A
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
B
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
C
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
A
Figure 5.
In this patient with a slow heart rate of 42 BPM, note the decreased image quality of the (A) standard short axis FIESTA Cine in 4 min. tapping time compared to the (B) short axis Sonic DL™ Cine, 3 RR with 1 min. tapping time, and (C) short axis Sonic DL™ Cine, 1 R-R with 40 sec. tapping time.
B
Figure 5.
In this patient with a slow heart rate of 42 BPM, note the decreased image quality of the (A) standard short axis FIESTA Cine in 4 min. tapping time compared to the (B) short axis Sonic DL™ Cine, 3 RR with 1 min. tapping time, and (C) short axis Sonic DL™ Cine, 1 R-R with 40 sec. tapping time.
C
Figure 5.
In this patient with a slow heart rate of 42 BPM, note the decreased image quality of the (A) standard short axis FIESTA Cine in 4 min. tapping time compared to the (B) short axis Sonic DL™ Cine, 3 RR with 1 min. tapping time, and (C) short axis Sonic DL™ Cine, 1 R-R with 40 sec. tapping time.
A
Figure 7.
With Sonic DL™ Cine 6 R-R, it is possible to achieve rapid temporal resolution and maintain spatial resolution as demonstrated in this (A) closed aortic valve and (B) open aortic valve.
B
Figure 7.
With Sonic DL™ Cine 6 R-R, it is possible to achieve rapid temporal resolution and maintain spatial resolution as demonstrated in this (A) closed aortic valve and (B) open aortic valve.
D
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
E
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
F
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
G
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
1. Desai DS, Hajouli S. Arrhythmias. StatPearls. 2023. PMID: 32644349.
A
Figure 1.
A 76-year-old male with shortness of breath, abnormal echocardiogram and large burden premature ventricular contractions referred to CMR for evaluation of cardiomyopathy. Sonic DL™ 1 R-R has significantly helped to reduce the artifacts (arrows) in a very short scan time. (A) Short axis FIESTA Cine, 1:40 min.; (B) short axis Sonic DL™ Cine, 3 R-R, 40 sec.; (C) short axis Sonic DL™ Cine, 1 R-R, 21 sec; (D) LVOT Sonic DL™ Cine; and (E) LVOT FIESTA Cine.
B
Figure 1.
A 76-year-old male with shortness of breath, abnormal echocardiogram and large burden premature ventricular contractions referred to CMR for evaluation of cardiomyopathy. Sonic DL™ 1 R-R has significantly helped to reduce the artifacts (arrows) in a very short scan time. (A) Short axis FIESTA Cine, 1:40 min.; (B) short axis Sonic DL™ Cine, 3 R-R, 40 sec.; (C) short axis Sonic DL™ Cine, 1 R-R, 21 sec; (D) LVOT Sonic DL™ Cine; and (E) LVOT FIESTA Cine.
C
Figure 1.
A 76-year-old male with shortness of breath, abnormal echocardiogram and large burden premature ventricular contractions referred to CMR for evaluation of cardiomyopathy. Sonic DL™ 1 R-R has significantly helped to reduce the artifacts (arrows) in a very short scan time. (A) Short axis FIESTA Cine, 1:40 min.; (B) short axis Sonic DL™ Cine, 3 R-R, 40 sec.; (C) short axis Sonic DL™ Cine, 1 R-R, 21 sec; (D) LVOT Sonic DL™ Cine; and (E) LVOT FIESTA Cine.
D
Figure 1.
A 76-year-old male with shortness of breath, abnormal echocardiogram and large burden premature ventricular contractions referred to CMR for evaluation of cardiomyopathy. Sonic DL™ 1 R-R has significantly helped to reduce the artifacts (arrows) in a very short scan time. (A) Short axis FIESTA Cine, 1:40 min.; (B) short axis Sonic DL™ Cine, 3 R-R, 40 sec.; (C) short axis Sonic DL™ Cine, 1 R-R, 21 sec; (D) LVOT Sonic DL™ Cine; and (E) LVOT FIESTA Cine.
E
Figure 1.
A 76-year-old male with shortness of breath, abnormal echocardiogram and large burden premature ventricular contractions referred to CMR for evaluation of cardiomyopathy. Sonic DL™ 1 R-R has significantly helped to reduce the artifacts (arrows) in a very short scan time. (A) Short axis FIESTA Cine, 1:40 min.; (B) short axis Sonic DL™ Cine, 3 R-R, 40 sec.; (C) short axis Sonic DL™ Cine, 1 R-R, 21 sec; (D) LVOT Sonic DL™ Cine; and (E) LVOT FIESTA Cine.
A
Figure 8.
A 56-year-old claustrophobic patient referred for aortic insufficiency evaluation. For a faster acquisition, (A-C) Sonic DL™ Cine 3 R-R was used. (D, E) 4D Flow demonstrates the aortic regurgitant jet.
B
Figure 8.
A 56-year-old claustrophobic patient referred for aortic insufficiency evaluation. For a faster acquisition, (A-C) Sonic DL™ Cine 3 R-R was used. (D, E) 4D Flow demonstrates the aortic regurgitant jet.
E
Figure 8.
A 56-year-old claustrophobic patient referred for aortic insufficiency evaluation. For a faster acquisition, (A-C) Sonic DL™ Cine 3 R-R was used. (D, E) 4D Flow demonstrates the aortic regurgitant jet.
C
Figure 8.
A 56-year-old claustrophobic patient referred for aortic insufficiency evaluation. For a faster acquisition, (A-C) Sonic DL™ Cine 3 R-R was used. (D, E) 4D Flow demonstrates the aortic regurgitant jet.
D
Figure 8.
A 56-year-old claustrophobic patient referred for aortic insufficiency evaluation. For a faster acquisition, (A-C) Sonic DL™ Cine 3 R-R was used. (D, E) 4D Flow demonstrates the aortic regurgitant jet.




result
PREVIOUS
${prev-page}
NEXT
${next-page}
Subscribe Now
Manage Subscription
FOLLOW US
Contact Us • Cookie Preferences • Privacy Policy • California Privacy PolicyDo Not Sell or Share My Personal Information • Terms & Conditions • Security
© 2024 GE HealthCare. GE is a trademark of General Electric Company. Used under trademark license.

Melany Atkins, MD
Fairfax MRI Center,
Fairfax Radiological Consultants
—
Fairfax, VA
In Practice
Cardiac MR in less than 30 minutes with deep-learning technology
Cardiac MR in less than 30 minutes with deep-learning technology
by Melany Atkins, MD, Division Chief of Cardiac Imaging, Fairfax Radiological Consultants and Medical Director, Fairfax MRI Center, Fairfax, VA
Melany Atkins, MD
Fairfax MRI Center,
Fairfax Radiological Consultants
—
Fairfax, VA
Cardiac MR (CMR) can be a labor-intensive examination that typically requires relatively long acquisition times and repetitive, long patient breath-holds. Traditionally, this process involves acquiring segments of the cardiac cycle at a single-slice location over multiple heartbeats and stitching them together. These segmented images are then reconstructed to create a cine loop, or movie, for evaluation of the wall motion and function of the heart.
Both demand and indications for CMR have significantly increased over the last decade, in particular to address the need to assess patients with arrhythmias, including both atrial fibrillation and ventricular arrhythmia. It is estimated that up to 5% of the US population has an arrhythmia,1 although some patients with arrythmias don’t have symptoms, making it difficult to estimate the true prevalence. In these cases, CMR is used to evaluate the structure of the heart to determine the underlying cause for the arrhythmia.
Figure 1.
A 76-year-old male with shortness of breath, abnormal echocardiogram and large burden premature ventricular contractions referred to CMR for evaluation of cardiomyopathy. Sonic DL™ 1 R-R has significantly helped to reduce the artifacts (arrows) in a very short scan time. (A) Short axis FIESTA Cine, 1:40 min.; (B) short axis Sonic DL™ Cine, 3 R-R, 40 sec.; (C) short axis Sonic DL™ Cine, 1 R-R, 21 sec; (D) LVOT Sonic DL™ Cine; and (E) LVOT FIESTA Cine.
CMR imaging of a patient with an arrhythmia/irregular heartbeat can be very challenging. Many of these patients are also short of breath and laying flat exasperates their symptoms. There are also patients with slow heart rates; in these cases, the acquisition time is longer and may be more prone to motion artifacts.
To image the beating heart, fast imaging techniques using very short repetition and echo times are required, such as balanced steady-state free precession (bSSFP) or spoiled gradient echo sequences. Even with advances in scanner hardware and sequences, it is difficult to obtain a quality CMR exam in many patients with arrhythmias or those who cannot hold their breath and, as a result, the study often has suboptimal image quality. Concessions can be made, such as letting the patient breathe freely, then averaging out the motion and reading through the respiratory motion artifacts. Prospective gating can be employed, however, this may limit the ability to post-process the study for accurate volumetric and function measurements. These are paramount for clinical decisions regarding patient management, especially in heart failure patients.
A

B

C
D
E
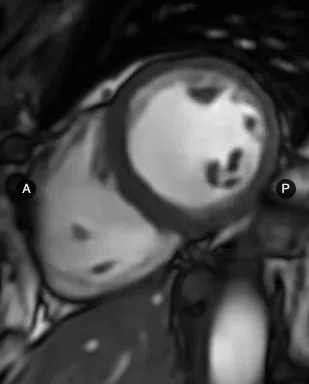
Figure 2.
A 76-year-old male patient with shortness of breath, claustrophobia and arrhythmia with an abnormal echocardiogram. Short axis cine images, (A) FIESTA Cine, (B) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R. In the 3-chamber view images, (D) FIESTA Cine image quality is marred by the severe arrhythmia, which obscures the aortic regurgitant jet. Both the (E) Sonic DL™ Cine, 3 R-R, and (C) Sonic DL™ Cine, 1 R-R, clearly provide better image quality in this patient.
The irony is that for these patients with arrhythmias – and in particular ventricular arrhythmias – the CMR study is needed to determine if their condition is due to structural or electrical issues so that treatment options can be pursued. Without a quality diagnostic study, the answer may be elusive.
A new deep-learning solution from GE HealthCare is helping to address these challenges in CMR. Sonic DL™ Cine acquires high-quality MR images up to 12 times faster than conventional methods, enabling cardiac imaging within a single heartbeat (1 R-R). In patients with arrhythmias, we can now acquire each slice of their heart in one heartbeat for effectively real-time imaging that allows for visualization of wall motion without artifact and obviates the need for the traditional segmental approach.
A
B
C
D
E
F
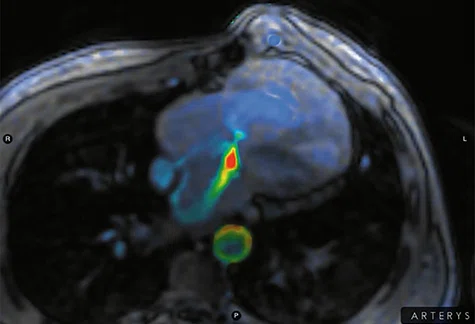
Figure 3.
A 17-year-old male patient with congenital heart disease and hypoplastic left heart syndrome referred for routine follow-up evaluation after bidirectional Glenn and fenestrated Fontan procedures. In complex congenital heart disease patients, rapid acquisition in different imaging planes are often needed to answer the clinical question. The entire axial stack was acquired in two 16 sec. breath-holds (A, B) FIESTA Cine; (C, D) Sonic DL™ Cine, 3 R-R; and (E, F) HLHS status post Fontan with (E) Sonic DL™ Cine, 3 R-R, and (F) 4D Flow.

A

B

C
D
E
F
G
Figure 4.
An 18-year-old male with Tetralogy of Fallot referred for CMR for routine follow-up status post pulmonic replacement. Echocardiogram demonstrated poor acoustic windows. (A) FIESTA Cine short axis; (B) Sonic DL™ Cine short axis, 3 R-R; (C) Sonic DL™ Cine 4 chambers, 3 R-R; (D) Axial 3D Heart; (E, F) 4D Flow; and (G) Sonic DL™ Cine RVOT.
In patients who cannot hold their breath, Sonic DL™ Cine enables capturing the image during a 1 R-R interval with respiratory triggering, so the patient can breathe freely. And, because Sonic DL™ Cine provides a novel rapid acceleration technique leveraging deep-learning image reconstruction that does not have the same limitations as conventional acceleration techniques, the total exam time is significantly shorter for all patients.
In an abstract presented at the Society for Cardiovascular Magnetic Resonance (SCMR) 2023 Scientific Sessions, we demonstrated a 50-75% reduction in scan time using a Sonic DL™ Cine research prototype compared to a standard FIESTA Cine acquisition. At Fairfax MRI Center with the commercial Sonic DL™ Cine solution, we’ve imaged over 100 patients with similar scan time reduction results.

A
B

C
Figure 5.
In this patient with a slow heart rate of 42 BPM, note the decreased image quality of the (A) standard short axis FIESTA Cine in 4 min. tapping time compared to the (B) short axis Sonic DL™ Cine, 3 RR with 1 min. tapping time, and (C) short axis Sonic DL™ Cine, 1 R-R with 40 sec. tapping time.

A

B
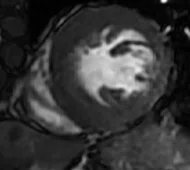
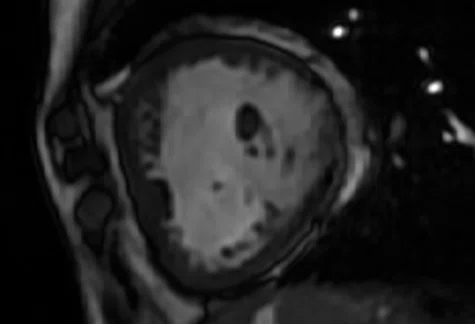
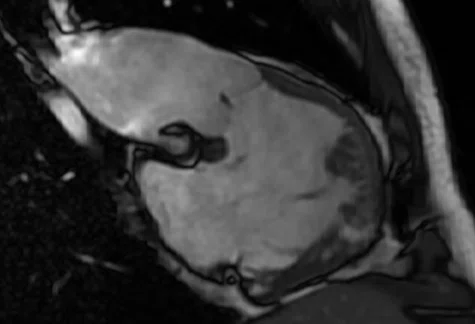
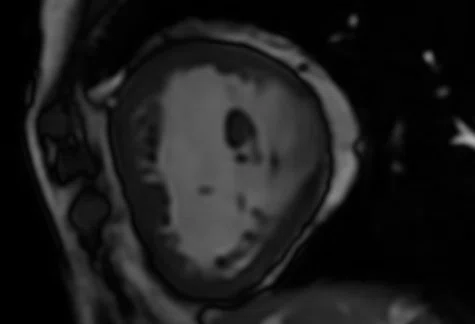
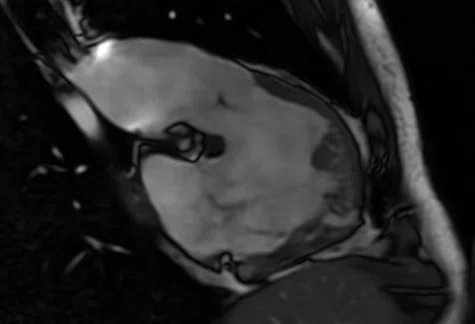
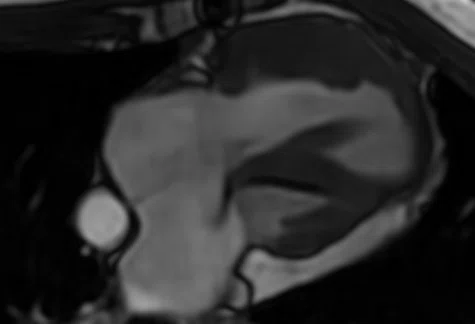
Figure 6.
Claustrophobic patients often cannot breath-hold. Respiratory triggering can be utilized in these patients. (A, B) Images were acquired with Sonic™ DL, 1 R-R, entire HLA stack in 1:20 min.
Sonic DL™ Cine is optimized at Fairfax MRI Center based on the patient’s condition. Our standard protocol is a three heartbeat (3 R-R), acquisition. In patients with arrhythmias or those who cannot hold their breath, we utilize the 1 R-R acquisition. While the 1 R-R acquisition has slightly lower temporal resolution and less spatial resolution than the 3 R-R acquisition, it has a much faster acquisition time and can be respiratory triggered.
As a result of our clinical evaluation of Sonic DL™ Cine, we have replaced all our standard FIESTA Cine acquisitions with the 3 R-R Sonic DL™ Cine acquisition. In some specific cases, we’ve used the 6 R-R acquisition for very fast temporal resolution with high spatial resolution that optimizes visualization of valve leaflets or mobile cardiac masses, which are thin structures and move rapidly. With Sonic DL™ Cine, our standard localizer scan has gone from a 6 second acquisition to a 1 second acquisition. Our total scan times have also been reduced by 50% since adjusting our routine protocols.

A

B
Figure 7.
With Sonic DL™ Cine 6 R-R, it is possible to achieve rapid temporal resolution and maintain spatial resolution as demonstrated in this (A) closed aortic valve and (B) open aortic valve.
The anatomy of patients with complex congenital heart disease is variable, often requiring additional imaging planes and sequences, which leads to long scan times. Our goal is for every patient – even the most complex congenital heart cases – to be scanned in under 30 minutes. For non-cine acquisitions, AIR™ Recon DL is utilized to further enhance spatial resolution and shorten scan time in all compatible sequences, such as single-shot PSIR, Double IR, T2, etc.
A standard CMR exam should not feel like a workout or pulmonary rehab for our patients. Longer scan times also lead to poor patient compliance and more difficulty breath-holding. With Sonic DL™ Cine, it is now possible to provide a more comfortable, shorter and less labor-intensive CMR exam for patients that is also reliable and repeatable, and provides the image quality, temporal resolution and spatial resolution needed to evaluate the beating heart confidently and accurately in all patients, regardless of their condition or heart rate.
DOWNLOAD ARTICLE HERE
