A
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
B
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
C
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
D
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
E
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
F
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
G
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
H
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
I
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
J
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
K
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
L
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.
Figure 2.
Sonic DL™ Cine can improve patient throughput in CMR examinations. Using Sonic DL™ Cine and AIR™ Recon DL together allow for a total exam time of less than 30 min.
A
Figure 3.
A 60-year-old male with low cardiac function and tachycardial atrial fibrillation. Patient was imaged with (A) FIESTA Cine with breath-hold, (B) Sonic DL™ Cine 1 R-R breath-hold and (C) Sonic DL™ Cine 3 R-R breath-hold.
B
Figure 3.
A 60-year-old male with low cardiac function and tachycardial atrial fibrillation. Patient was imaged with (A) FIESTA Cine with breath-hold, (B) Sonic DL™ Cine 1 R-R breath-hold and (C) Sonic DL™ Cine 3 R-R breath-hold.
C
Figure 3.
A 60-year-old male with low cardiac function and tachycardial atrial fibrillation. Patient was imaged with (A) FIESTA Cine with breath-hold, (B) Sonic DL™ Cine 1 R-R breath-hold and (C) Sonic DL™ Cine 3 R-R breath-hold.
1. von Knobelsdorff-Brenkenhoff F, Schulz-Menger J. Cardiovascular magnetic resonance in the guidelines of the European Society of Cardiology: a comprehensive summary and update. J Cardiovasc Magn Reson. 2023; 25(1):42.
2. ACR–NASCI–SPR PRACTICE PARAMETER FOR THE PERFORMANCE AND INTERPRETATION OF CARDIAC MAGNETIC RESONANCE IMAGING (MRI). Revised 2021 (Resolution 42). Available at: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/MR-Cardiac.pdf.
Orii M, Sone M, Osaki T, et al. Reliability of respiratory-gated real-time two-dimensional cine incorporating deep learning reconstruction for the assessment of ventricular function in an adult population. Int J Cardiovasc Imaging. 2023;39(5):1001-1011.




result
PREVIOUS
${prev-page}
NEXT
${next-page}
Subscribe Now
Manage Subscription
FOLLOW US
Contact Us • Cookie Preferences • Privacy Policy • California Privacy PolicyDo Not Sell or Share My Personal Information • Terms & Conditions • Security
© 2024 GE HealthCare. GE is a trademark of General Electric Company. Used under trademark license.

Makoto Orii, MD
Iwate Medical University
—
Iwate, Japan
In Practice
Reliable and rapid real-time 2D cine with deep-learning technology for robust free-breathing cardiac MR
Reliable and rapid real-time 2D cine with deep-learning technology for robust free-breathing cardiac MR
Makoto Orii, MD
Iwate Medical University
—
Iwate, Japan
Cardiac MR (CMR) is the gold standard for assessing the structure and function of the heart in cardiovascular disease.1,2 However, global adoption remains relatively low, in part due to lengthy exam times. The current acquisition speed of MR is too slow to capture the heart’s contraction in real time, requiring several heartbeats and multiple breath-holds. This process is time-consuming, prone to image quality degradation and exhausting for patients. Consequently, there is a pressing need to address the growing demand for fast, high-quality and comfortable CMR imaging.
The CMR imaging service at Iwate Medical University in Iwate, Japan, has experienced this uptick in demand for cardiac imaging. The facility previously performed one cardiac case per week on its two MR systems, the SIGNA™ Architect and SIGNA™ Artist. Today, the facility performs approximately four cases per week, primarily focused on non-ischemic cardiomyopathy. Additionally, Iwate performs one to two pediatric cardiac exams each week, measuring right ventricular volume, assessing pulmonary blood flow, and evaluating aortic flow velocity and pulmonary artery regurgitation using 2D phase-contrast (PC) MR imaging.
Iwate recently implemented Sonic DL™ Cine to address the most challenging MR cases, cardiac cine, and enable MR imaging of patients who couldn’t be effectively imaged before, namely those with arrythmias and those who cannot hold their breath. The technology, Sonic DL™ Cine, is a state-of-the-art, deep-learning-based technology that enables high-quality CMR in a single heartbeat. In June 2023, GE HealthCare announced the FDA clearance of Sonic DL™ Cine.
At Iwate, Sonic DL™ Cine has helped reduce CMR imaging from 5 minutes and 30 seconds with conventional scanning methods to less than 1 minute, without sacrificing diagnostic utility. “Thanks to Sonic DL™ Cine, scan times have been significantly reduced to just 41 seconds. Clinical evaluation confirmed that volumetric assessments, similar to those done using conventional methods, can be obtained without any drawbacks, making it feasible for clinical use without disadvantages,” said Makoto Orii, MD, Assistant Professor at Iwate Medical University.
Dr. Orii and colleagues published their initial evaluation of Sonic DL™ Cine with respiratory-triggered, free-breathing, compared to the current standard reference breath-hold 2D balanced steady-state free precession (bSSFP), or FIESTA Cine, in The International Journal of Cardiovascular Imaging.3 In addition to significantly shorter acquisition times comparing Sonic DL™ Cine with FIESTA Cine (41.0 ± 11.3 sec. vs. 327.6 ± 65.8 sec., respectively; p < 0.0001), there was no significant difference in the blood-to-myocardial contrast image quality scores between the two sequences. Further, compared to the FIESTA Cine sequence, Sonic DL™ Cine allowed for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters. The authors found Sonic DL™ Cine to be better than other short-axis techniques compared to FIESTA Cine in similar studies.
End-diastole
End-systole
FIESTA Cine breath-hold
Sonic DL™ Cine free-breathing
FIESTA Cine breath-hold
Sonic DL™ Cine free-breathing
A
B
C
D
E
F
G
H
I
J
K

L
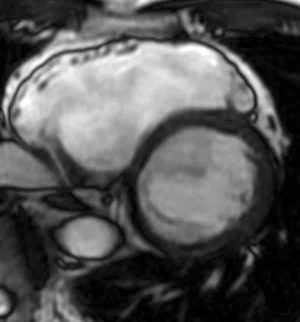
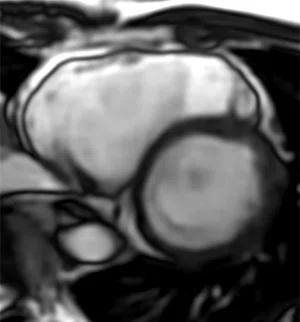
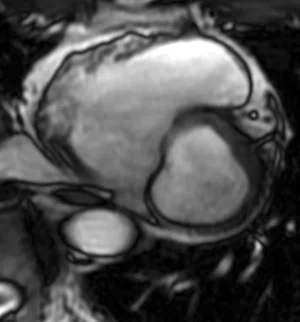
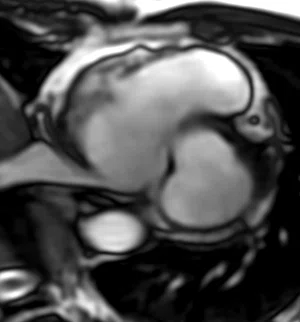
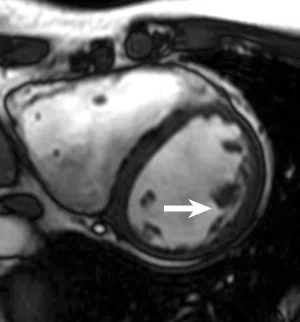
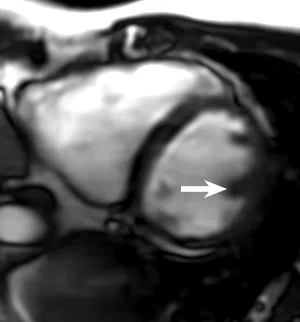
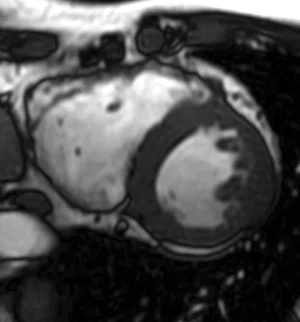
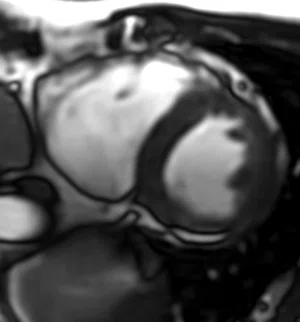
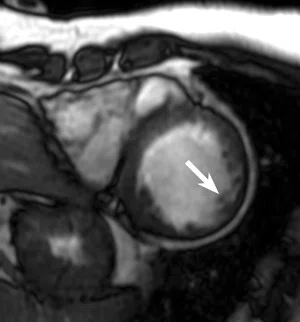
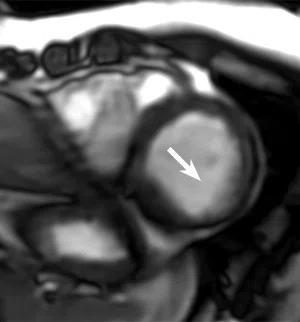
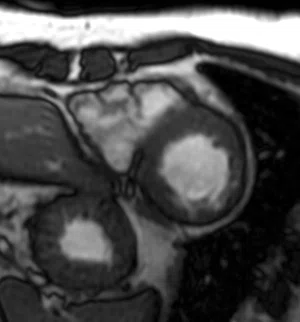
Figure 1.
Patient with hypertrophic cardiomyopathy was imaged using the conventional, breath-hold method, FIESTA Cine (bSSFP) and Sonic DL™ Cine with free-breathing. (A-D) Top row is basal portion, (E-H) middle row is the papillary muscle (mid) and (I-J) bottom row is the apex portion. (A, C, E, G, I, K) This representative case shows similar diagnostic image quality between FIESTA Cine and Sonic DL™ Cine with only subtle motion blurring and degradation of the papillary muscle edge delineation on Sonic DL™ Cine (white arrows) in a significantly shorter scan time (see Table 2) and allowing for an accurate evaluation of biventricular volumes and ejection fraction, including right ventricular parameters.

Table 1.
Acquisition parameters comparing FIESTA Cine to Sonic DL™ Cine.

Table 2.
Comparison of image quality and acquisition time between FIESTA Cine with breath-hold and Sonic DL™ Cine with free-breathing. Note the significantly shorter acquisition time for Sonic DL™ Cine. Contrast, edge and motion were rated on a scale of 1-5: 1=non-diagnostic, 2=suboptimal but diagnostic for volumetric analysis, 3=adequate, 4=good and 5=excellent.3

Figure 2.
Sonic DL™ Cine can improve patient throughput in CMR examinations. Using Sonic DL™ Cine and AIR™ Recon DL together allow for a total exam time of less than 30 min.
Fast, free-breathing cardiac scans
Sonic DL™ Cine allows Dr. Orii to capture free-breathing scans, which helps him image adults and children who can’t hold their breath due to factors such as congenital heart conditions requiring right ventricular evaluation.
The technology offers benefits over cardiac ultrasound, which often doesn’t clearly assess the right ventricle of the heart. Furthermore, many individuals who suffer from sleep apnea fall asleep during the longer conventional MR exam, which could result in blurred images due to the lack of breath-hold, making diagnoses difficult. Dr. Orii believes that free-breathing imaging with Sonic DL™ Cine can be applied effectively in these patients, expanding the utility of MR cardiac imaging.
Sonic DL™ Cine’s ability to capture rapid cine imaging in more patients has enabled shorter scans and higher patient volumes. Currently, Iwate schedules patients in 1 hour timeslots for CMR imaging, but Dr. Orii expects to shorten these exams to just 30 minutes with Sonic DL™ Cine. “We believe this is possible by shortening the time required for cine imaging, which was a time-consuming aspect in the conventional method,” he said.
However, Dr. Orii notes that free-breathing imaging is not suitable for all examinations. “In addition to free-breathing imaging, we are also exploring methods where imaging is conducted with a single breath-hold to acquire the whole heart. We are actively studying and evaluating imaging parameters for this breath-hold technique,” he said.
While volumetric assessments were previously infrequently performed with Cine MR, these exams are essential for pediatric patients. Therefore, improving the efficiency of Cine MR is crucial for meeting these demands and streamlining the overall CMR examination process.
“We place a strong emphasis on the ability to easily acquire cine images within the examination workflow. Therefore, reducing imaging time is a must. While it would be ideal to capture short-duration images with free-breathing, if volumetric assessment is required, there is also the option to prioritize image quality with multiple breath-holds,” he said.
Iwate is also testing a breath-hold technique that acquires each slice in three heartbeats.

A

B

C
Figure 3.
A 60-year-old male with low cardiac function and tachycardial atrial fibrillation. Patient was imaged with (A) FIESTA Cine with breath-hold, (B) Sonic DL™ Cine 1 R-R breath-hold and (C) Sonic DL™ Cine 3 R-R breath-hold.
Speed without sacrifice
According to Dr. Orii, it’s important to categorize the underlying causes of a patient’s heart arrhythmia. For ventricular and occasional premature contractions, conventional imaging methods typically do not result in significant image degradation. However, in cases where R-R intervals vary significantly, such as in atrial fibrillation, there is a notable decrease in image quality. “For such patients, the conventional method may not be feasible, but Sonic DL™ Cine has significantly improved image quality in these cases,” he said.
Iwate Medical University is also considering variations in the R-R interval in addition to conventional MR imaging. “We’re continuously exploring ways to accelerate cine imaging. Previously, we conducted investigations using parallel imaging techniques, but with the transition to Sonic DL™ Cine, the image quality has improved significantly,” said Dr. Orii.
Initially, parallel imaging techniques allowed for short-duration imaging during free breathing and received very positive evaluations. However, there were instances of image blurring when using these techniques. In a study focused on post-surgery patients with congenital heart conditions, the results indicated that left ventricular volume remained unchanged between the conventional and parallel imaging methods. However, post-surgery patients often exhibit right ventricular expansion and the right ventricle tends to exhibit blurring during motion with parallel imaging techniques, resulting in significant differences in values between both.
Subsequently, Dr. Orii and his colleagues conducted evaluations of volume assessments using Sonic DL™ Cine. “Sonic DL produces images with high SNR and sharpness. With Sonic DL™ Cine, we found we could assess left ventricular and right ventricular volumes and contractility in a manner similar to the conventional method,” Dr. Orii said.
Future generations of Sonic DL™ are expected to be compatible with 2D and 3D sequences across all clinical areas. Dr. Orii believes if Sonic DL™ Cine is combined with an image reconstruction quality enhancement technology, it could help address the image quality impairment of endocardial edge definition and motion artifacts.
DOWNLOAD ARTICLE HERE
