A
Figure 2.
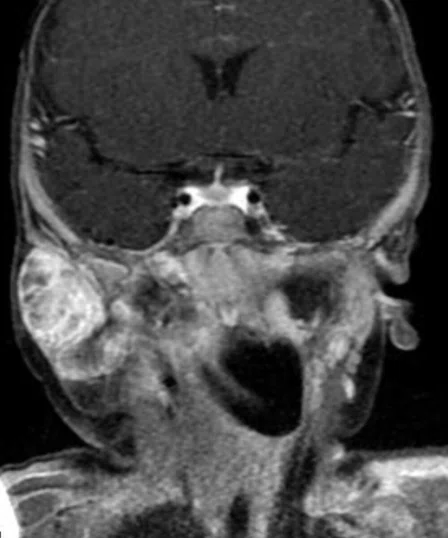
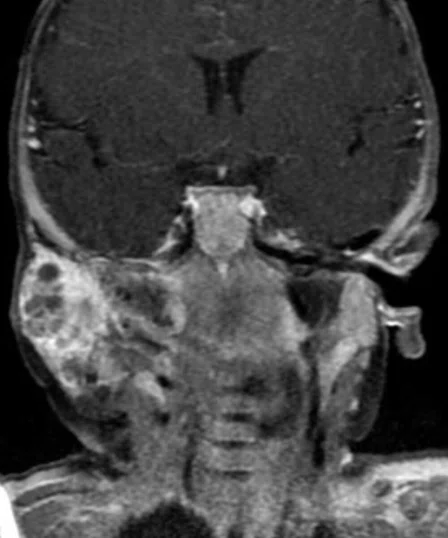
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
B
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
C
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
D
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
E
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
F
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
A
Figure 1.
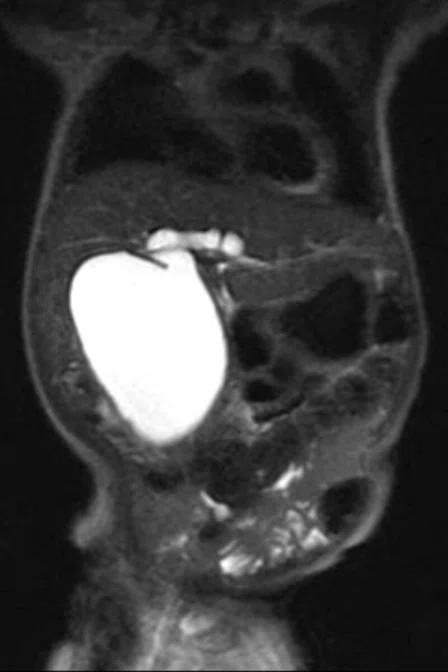
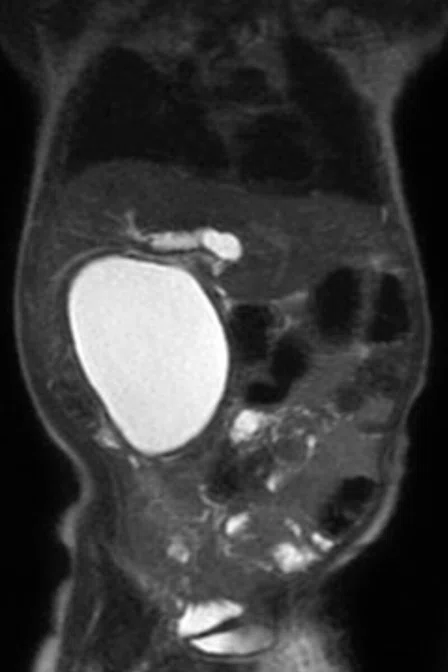
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
B
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
C
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
D
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
E
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
F
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
G
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
H
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
G
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
H
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.




result
PREVIOUS
${prev-page}
NEXT
${next-page}
Subscribe Now
Manage Subscription
FOLLOW US
Contact Us • Cookie Preferences • Privacy Policy • California Privacy PolicyDo Not Sell or Share My Personal Information • Terms & Conditions • Security
© 2024 GE HealthCare. GE is a trademark of General Electric Company. Used under trademark license.

Amaresh Ranchod, MB BCh
Netcare Waterfall City Hospital
Midrand, South Africa

Samantha Palliam, MB ChB
Netcare Waterfall City Hospital
Midrand, South Africa

Kumeshnie Kollapen, MB ChB
Netcare Waterfall City Hospital
Midrand, South Africa
Michael Maila, RT(R)
Netcare Waterfall City Hospital
Midrand, South Africa
IN PRACTICE
Upgrade delivers imaging excellence
Upgrade delivers imaging excellence
Amaresh Ranchod, MB BCh
Netcare Waterfall City Hospital
Midrand, South AfricaSamantha Palliam, MB ChB
Netcare Waterfall City Hospital
Midrand, South AfricaKumeshnie Kollapen, MB ChB
Netcare Waterfall City Hospital
Midrand, South AfricaMichael Maila, RT(R)
Netcare Waterfall City Hospital
Midrand, South AfricaWhat began as a single practice in Springs, South Africa, has grown into a multi-site radiology group serving the residents in and around the Johannesburg-Pretoria area. National Radiology Services, Inc., (NRS) has invested in a full spectrum of state-of-the-art imaging technology. Recently NRS upgraded its Optima™ MR360 1.5T MR system to a SIGNA™ Explorer at Netcare Waterfall City Hospital in Midrand.
What began as a single practice in Springs, South Africa, has grown into a multi-site radiology group serving the residents in and around the Johannesburg-Pretoria area. National Radiology Services, Inc., (NRS) has invested in a full spectrum of state-of-the-art imaging technology. Recently NRS upgraded its Optima™ MR360 1.5T MR system to a SIGNA™ Explorer at Netcare Waterfall City Hospital in Midrand.
Netcare Waterfall City Hospital, a multi-disciplinary hospital with a Level III 24-hour ER, provides a range of services — from a bariatric center to epilepsy monitoring and robotic-assisted surgery for localized prostate, bladder and kidney cancer. Yet, it is the pediatric services that often set this hospital apart, with a pediatric and neonatal ICU, and a pediatric high care ward.
In 2012, the hospital installed an Optima™ MR360 for advanced MR imaging. However, as technology advanced, the hospital found its MR system lagged behind the competition. Although the hospital had a very good reputation, it was losing referrals to a nearby hospital with a new MR system.
Amaresh Ranchod, MB BCh, a diagnostic radiologist, explains that the hospital and radiology group looked at several options, including buying new or upgrading the existing scanner. He knew replacing the MR system would incur more cost and downtime.
“The upgrade was the middle option that we hoped would give us more value,” Dr. Ranchod says.
“We also felt the upgrade would be the best option to shorten exam times and improve image quality,” adds Samantha Palliam, MB ChB, a diagnostic radiologist at Netcare Waterfall City Hospital who often handles oncology and pediatric cases.
Excellence in pediatric imaging
Many children are under general anesthesia for an MR exam, and the clinicians want the duration of both the scan and the anesthesia to be as short as possible.
“Imaging a patient in the shortest amount of time with all the sequences needed is ideal for these children,” Dr. Palliam adds. “There are many advantages for pediatric MR with the new upgrade.”
For example, MAGnetic resonance imaging Compilation (MAGiC) allows her to scan up to eight contrasts in one 5½ minute scan and then change TE, TR and T1 after the exam. Dr. Palliam also has access to parametric maps, including T1, T2, R1, R2 and PD.
“It is really important to be as quick as possible without compromising image quality,” Dr. Palliam says. “We are still adjusting our protocols. The system and sequences are not yet as fast as they can be, but we plan to improve them over the next year. Overall, there has definitely been an improvement in image quality.”
Dr. Palliam recalls a recent case of a 33-month-old child with a cystic lesion in the gallbladder fossa (see Figure 1). Initially, there was concern that the lesion involved another organ, such as the liver or pancreas. Ultrasound was indeterminate, so an MRCP exam was scheduled.
A
B

C

D

E

F
G
H
Figure 1.
A 33-month-old child with a cystic lesion in the gallbladder fossa. An MRCP exam was scheduled, however, there were issues with breathing and respiration. Auto Navigator for free-breathing was utilized to obtain diagnostic-quality images of a lesion that is highly suggestive of a choledochal cyst with a Todani type II classification. (A-D) SSFSE with breath hold. (E-H) Free-breathing exam using Auto Navigator; (E, F) axial T2 FrFSE; (G) 3D axial FSPGR Dual Echo; and (H) 3D MRCP.
“During the exam, we tried to do an MRCP sequence, however, we were still having issues with respiration and breathing artifacts,” she explains. Fortunately, the SIGNA™ Explorer with SIGNA™Works includes Auto Navigator, a free-breathing approach to combat respiratory motion in the body that uses a navigator pulse to track the motion of the diaphragm. By automatically placing the navigator tracker pulse over the right hemidiaphragm, the acquisition is synchronized to the patient’s breathing pattern and thus minimizes respiratory ghosting artifacts. Real-time adjustment allows threshold levels to be modified during the acquisition — eliminating failures due to changes in respiratory patterns of the patient.
As a result of using Auto Navigator in the MRCP exam, Dr. Palliam was able to determine the lesion was highly suggestive of a choledochal cyst with a Todani type II classification.
In Dr. Palliam’s opinion, this case demonstrates the advantage of the SIGNA™ Explorer with sequences that can more easily augment breathing patterns, minimize artifacts and deliver the image quality needed for diagnosis.
Kumeshnie Kollapen, MB ChB, has an interest in pediatric radiology and says the services they provide are quite different from other hospitals because of the underlying high quality of imaging devices and clinical expertise. She recently joined the practice serving Netcare Waterfall City Hospital.
“Ideally, we want to always optimize image quality in children and with the new hardware, software and sequences we are able to do that. With optimal quality, we can avoid repeating sequences and that’s important because we don’t want the pediatric patients under anesthesia for too long.”
Dr. Kumeshnie Kollapen
The T1 PROPELLER sequence delivers excellent resolution and addresses patient motion to provide her with the information she needs to assess the normal midline pediatric CNS structures. While 3D Cube may be a longer scan than T2 FLAIR, it is important to get the information needed in cases where there are subtle changes in brain white matter, such as hypoxic injuries.
“We have the tools to tailor each case to the individual pediatric patient,” Dr. Kollapen adds.
In one case, a six-month-old boy presented with swelling on the right side of the face (see Figure 2). An initial ultrasound helped her diagnose a complex cystic lesion demonstrating multi-compartmental involvement of the right side of the neck, predominantly involving the preauricular and submandibular regions. However, an MR exam was ordered to further determine the type of lesion.
A
B
C
D
E
F
G
H
Figure 2.
A six-month-old boy with swelling on the right side of the face. (A-D) The lesion was predominantly hypointense on T1 FatSat images, including (D) IDEAL, with scattered areas of hyperintense signal. (E, F) Coronal T2 STIR showed the lesion was encased by the branches of the external carotid artery and there were multiple fluid levels. (G, H) TRICKS helped depict the different phases of enhancement in a large, complex lobulated soft tissue mass lesion seen arising from the right parotid gland.
Using TRICKS on SIGNA™ Explorer, Dr. Kollapen was able to appreciate the different phases of enhancement that provided additional information to help her diagnose a vero-lymphatic malformation. The mass demonstrated persistent delayed enhancement.
“The lesion was predominantly hypointense on T1 with scattered areas of hyperintense signal, which may represent a proteinaceous or hemorrhagic component,” she explains. “The lesion encased part of the branches of the external carotid artery and there were multiple fluid levels that were best appreciated with the T2 acquisition.”
Prostate imaging
With the upgrade to SIGNA™ Explorer, Dr. Ranchod got the value he hoped for in body and prostate imaging. In MSK imaging, he routinely uses FSE Flex for consistent and reliable FatSat. With one scan, he can obtain a fluid-sensitive sequence that is useful in MSK cases. In prostate imaging, he has discovered multiple benefits since the upgrade.
The LAVA sequence has improved, particularly in the post-contrast phase. And, since diffusion imaging with ADC is an important sequence for all prostate cancer MR exams, Dr. Ranchod now has access to MAGiC DWI.
“MAGiC DWI allows us to get the high diffusion value we need without scanning, so that reduces exam times to some extent. But, the overall quality is better and that makes a difference.”
Dr. Amaresh Ranchod
In one case, a patient had a rising PSA that spiked. The prior random systematic biopsy was negative. Dr. Ranchod detected a lesion suspicious for cancer (PI-RADS v2.1) in the left anterior peripheral zone at the apex. The lesion was missed on the initial non-directed biopsy; guided biopsy post-MR confirmed prostate carcinoma.
“Now, we can direct the urologist to the target lesion by fusing MR with ultrasound for precise image guidance,” he says.
Improvement across the board
The SIGNA™ Explorer has improved nearly all exams, adds Michael Maila, RT(R), Head Radiographer at Netcare Waterfall City Hospital. He is impressed by many of the new sequences, although it is the selection of coils that really impacts his daily routine.
“It is very easy to position the patient with the 16 channel Flex Coils compared to the hard shell fixed coils. The new system is impressive. We have the same user-friendly interface, but with more options and more sequences. That gives us an advantage, especially when combined with the new coils.”
Michael Maila
By upgrading to the SIGNA™ Explorer, technologists can now more successfully perform challenging cases. It has expanded the clinical capabilities of the site considerably and, along with the increase in image quality, will enable Netcare Waterfall City Hospital to deliver excellence in MR imaging.
